UPDATE: On 4 July 2019, the Core Group will submit a “TABLING REV 1” version of their resolution on “Access to medicines and vaccines in the context of the right of everyone to the enjoyment of the highest attainable standard of physical and mental health” for consideration by the 41st session of the Human Rights Council on 11 July 2019. The new text can be found here:
HRC 41 – Access to medicines and vaccines – final tabling version
*(The author thanks Vitor Ido, South Centre, for his detailed notes of the first round of informal consultations held on 27 June 2019.)
On Monday, 1 July 2019, the Core Group (Brazil, China, Egypt, Indonesia, India, Senegal, South Africa and Thailand) circulated a revised version (REV 1) of their resolution on “Access to medicines and vaccines in the context of the right of everyone to the enjoyment of the highest attainable standard of physical and mental health” for consideration by the 41st session of Human Rights Council (HRC). This revised text is based on comments received at the first informal held in Room XXIV on 27 June 2019 from 15:00 to 16:30.
In terms of a concrete ask to the High Commissioner for Human Rights, Michelle Bachelet, the Core Group has requested the following:
To convene, before the forty-fourth sixth session of the Human Rights Council, a full-day intersessional seminar on good practices, key challenges and new developments relevant to access to medicines and vaccines as one of the fundamental elements of the right of everyone to the enjoyment of the highest attainable standard of physical and mental health, in coordination with the World Health Organization;
The access to medicines resolution is a triennial exercise dating back to 2001. In 2016, the 32nd session of the HRC “adopted a far-reaching resolution on access to medicines which provides the Human Rights Council a strong mandate to examine the relationship between international trade agreements, intellectual property rights obligations and their implications on access to medicines – through the prism of human rights.” (Source: Knowledge Ecology International, Human Rights Council adopts watershed resolution on Access to Medicines). Based on the mandate of this resolution, the Human Rights Council convened an access to medicines panel at its 34th session in March 2017 and invited Ruth Dreifuss and Justice Michael Kirby to present the findings of the Report of the United Nations High-Level Panel on Access to Medicines to the Council.
On Monday, 24 June 2019, the Core Group circulated a zero draft of their access to medicines and vaccines resolution. The 2019 text included references to the WHO transparency resolution (WHA72.8), the WHO Cancer resolution (WHA70.12), the WHO Cancer Report, Political Declaration of the High-Level Meeting of the General Assembly on Antimicrobial Resistance, Political Declaration of the Third High-Level Meeting of the General Assembly on the prevention and control of non-communicable diseases, Political Declaration of the High-Level Meeting of the General Assembly on the fight against tuberculosis, the WHO Road Map for Access to Medicines, Vaccines and other Related Health Products 2019-2023, and the 2018 Astana Declaration on Primary Health Care.
During the first informal (27 June 2019), Switzerland and Australia specifically called for the deletion of operative paragraph 5 of the resolution which referenced “delinkage”:
Reiterates the call upon States to continue to collaborate, as appropriate, on models and approaches that support the delinkage of the cost of new research and development from the prices of medicines, vaccines and diagnostics for diseases that predominantly affect developing countries, including emerging and neglected tropical diseases, so as to ensure their sustained accessibility, affordability and availability and to ensure access to treatment for all those in need;
In relation to operative paragraph 5, Australia made the following comment: “While we prefer deletion of this paragraph, we could also support deletion of ‘delinkage of costs of new’ and after development ‘from the prices'”. Brazil, on behalf of the Core Group, noted that the language contained in operative paragraph 5 on delinkage is agreed language from resolution A/HRC/32/L.23/Rev.1 (adopted in 2016). Consequently, this language on delinkage has been preserved in the 1 July 2019 (REV 1) text.
Vitor Ido (South Centre) provided the following insightful observations from the first informal:
“The European Union, Japan, Australia and Switzerland proposed numerous changes, mostly on already consolidated language. Australia explicitly said that “it is our view that IP places a positive role in rewarding and incentivizing innovation”. Switzerland mentioned multiple times that various non-addressed factors impact access to medicines and those were not addressed. Japan opposed discussions outside of WHO and raised concerns about the language, asking for multiple deletions. The EU proposed various changes including deletion of: “that aims to promote new thinking on innovation and access to medicines and to secure an enhanced and sustainable basis for needs-driven essential health research and development” and“avoid that exclusively-market driven approaches do not address”.”
“The two preambular paragraphs on the Doha Declaration and TRIPS Amendment were generally accepted. References to “alternative frameworks” for innovation were countered by such delegations. With different degrees of discontent, they opposed language referring to the UN High-Level Panel on Access to Medicines. The EU, Japan and Australia also opposed cherry-picking provisions from the WHO Roadmap”.
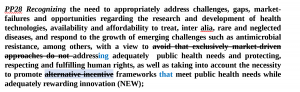
Paragraph 28 of the preamble (PP28) received intense scrutiny from the European Union, Japan, Switzerland and Australia. The text in the zero draft reads:
PP28 Recognizing the need to appropriately address challenges, gaps, market-failures and opportunities regarding the research and development of health technologies, availability and affordability to treat, inter alia, rare and neglected diseases, and respond to the growth of emerging challenges such as antimicrobial resistance, among others, with a view to avoid that exclusively market-driven approaches do not address adequately public health needs, as well as taking into account the necessity to promote alternative incentive frameworks to meet public health needs while adequately rewarding innovation (NEW);
In response to this language on alternative incentive frameworks, Japan noted,”There is no common understanding regarding alternative incentive frameworks. What kinds are available and should be promoted?”
Switzerland proposed to delete “emerging” before the word “challenges” and requested to delete ““with a view to avoid that exclusively market-driven approaches” noting that this was an “incorrect assumption”. Switzerland also supported the deletion of the language containing references to “alternative incentive frameworks”.
The European Union stated: “We understand the idea of problems of markets, and also the case for “rare diseases”. As compromise, we suggest: “with a view to [delete: avoid that exclusively-market driven approaches do not address] address adequately public health needs and human rights, and well as taking into account the necessity to promote alternative and complementary incentive frameworks”.
Australia chimed in: “We align with views of Japan and Switzerland, and the EU’s proposal could also satisfy..but we first need to check with capital.”
To see the resulting handiwork of this drafting exercise, please see the following image:
In the REV 1 text from 1 July 2019, the language on delinkage remains unchanged in spite of the recommendations of Australia and Switzerland.
5. Reiterates the call upon States to continue to collaborate, as appropriate, on models and approaches that support the delinkage of the cost of new research and development from the prices of medicines, vaccines and diagnostics for diseases that predominantly affect developing countries, including emerging and neglected tropical diseases, so as to ensure their sustained accessibility, affordability and availability and to ensure access to treatment for all those in need;
To compare the final tabling text, the REV 1 text and the zero draft please see the following links:
HRC 41 – Access to medicines and vaccines – final tabling version
CDH 41 – Access to medicines and vaccines – Rev1
RES-HRC-41-Access-to-medicines-ZERO-DRAFT.docx
The second informal will take place on Tuesday, 2 July 2019 from 14:30 to 16:00 in Room XXV of the UN Palais des Nations.