Bayh-Dole cases involving royalty free or march-in rights
1997 Cellpro case
This was a strong case involving two competing medical devices, both invented on NIH grants, and a bad ending. The NIH rejection of the Cellpro march-in request led to the bankruptcy of Cellpro, and the elimination of its bone marrow device, which was preferred by some some oncologists. The NIH was reportedly surprised about the demise of the Ceprate system and the outcome in general, as reported by Bill Richards in the Wall Street Journal in 1999. One benefit of the march-in case was that the NIH did not allow Johns Hopkins to enforce an injunction against the sale of the Ceprate system until the competing medical device was approved by the FDA.
- 1997, March 2. Petition from Lloyd Cutlter and former Senator Birch Bayh, on behalf of Cellpro, requesting the NIH use march-in rights on patents held by Johns Hopkins, infringed by Cellpro’s Ceprate medical device.
- 1997. August 1. Decision by Harold Varmus rejecting of the March-in petition, and the press release and media background memorandum.
- Several additional documents from NIH FOIA requests on the Cellpro case, here.
- 1999. Bill Richards, Baxter Beat CellPro in Court, But Some Say Dying Patients Lost, Wall Street Journal. August 6, 1999.
- 2002. Avital Bar-Shalom and Robert Cook-Deegan, Patents and Innovation in Cancer Therapeutics: Lessons from CellPro, Milbank Q. 2002 Dec; 80(4): 637–676., doi: 10.1111/1468-0009.00027. PMCID: PMC2690134
- 2012. Blog focusing on Birch Bayh’s competing interests and evolving views, August 24, 2012,
1999, June 22. Ventana Medical Systems march-in request for patent for fluorescent in situ hybridization (FISH) tests.
Ventana Medical Systems, Inc (later a division of Roche Diagnostics) petitioned the Bill Richardson, the Secretary of the U.S. Department of Energy, to use the government’s rights in patents held by the University of California patents that had been exclusively licensed to Vysis. The relevant patent was U.S. patent number 5,447,841, titled “Methods for chromosome-specific staining,” related to blocking DNA which is used in most in-situ hybridization (ISH) assays to chromosomal DNA. The inventors were Joe W. Gray and Daniel Pinkel, then working for the Lawrence Liver more National Laboratory, operated by the University of California. The patent contained this declaration of federal rights.
The United States Government has rights in this invention pursuant to Contract No. W-7405-ENG-48 between the U.S. Department of Energy and the University of California, for the operation of Lawrence Livermore National Laboratory.
The technology was developed entirely at the Energy Department Laboratory and the patent was assigned to the Regents Of The University Of California. The University of California has granted an exclusive license was granted to Vysis, a subsidiary of Abbott laboratories that makes genetic tests for cancer, prenatal disorders, microarrays, and other equipment used by medical and biotechnology researchers. The parties settled the dispute, after a 30-month fact-finding process determination with DOE, with the Ventana/Roche obtaining a license.
1999. Request that HHS regarding ddI.
On February 16, 1999, a Thai NGO, Access to Treatment, wrote a letter to Donna Shalala, Secretary to the Health and Human Services Department, asking for a review of the pricing of ddI, a treatment for HIV that was invented by NIH researchers and licensed to BMS. The Thai NGOs wanted HHS to grant Thailand the right to manufacture generic versions of the drug. On April 20, 1999, the Thai NGO received a reply to their February 16, 1999 letter to Donna Shalala. The reply was written by Dana Delman, a Policy Analyst for the US FDA Executive Secretariat. She stated that “neither FDA nor other segments of the US Federal Government have control over the pricing of drugs sold in the United States, let alone overseas,” and that “marketing exclusivity through the use of patent laws in this country has been an important stimulus to the development of new products to treat a variety of diseases.”
1999. Request that NIH enter into agreement with the WHO regarding use of royalty free rights in patents.
On September 3, 1999, Ralph Nader, James Love and Robert Weissman wrote a letter to NIH Director Harold Varmus urging the NIH to provide the World Health Organization with access to U.S. government-funded medical inventions.
- The NIH should enter into an agreement with the WHO that would permit the WHO to use US government intellectual property rights for public health initiatives. The NIH should specify the terms under with the WHO could use US government intellectual property rights, to ensure that the public interest is served.
- In those cases where the US government can now give the WHO rights to health care inventions under 37CFR404.7 and 37CFR401.5, the WHO should be authorized to use those rights.
- The US government should revise its grant and contract practices so that all new grants and contracts reference the WHO’s rights to use patents, under 37CFR401.5.
- The NIH should ask its general counsel to determine the scope of the NIH’s rights to government funded university and small business inventions under 37CFR401.14, and to the extent appropriate, engage the WHO, US AID or other international organizations or US agencies to use these rights to expand treatment opportunities for the poor.
On October 21, 1999, Dr. Varmus wrote back to Nader, Love and Weissman, rejecting the proposal for a “standardized transfer of manufacturing the distribution rights to the WHO or any other nonprofit organization, but welcomed “further discussions with WHO on what can be done to assist developing countries with health care needs.”
As you have pointed out, the Government has a royalty-free license to practice and have practiced an invention it owns or has funded on behalf of the United States and on behalf of a foreign government or international organization pursuant to a treaty or other agreement with the United States. This royalty-free license provides the Government with no-cost use of a technology it invented or funded. It does not provide rights or access to a licensee’s final product. The Government use contemplated by this provision has been interpreted generally to include research use, although its full scope has not been determined. Providing the owner of the technology (licensor) freedom to do further research is a common and reasonable provision of exclusive licenses. To our knowledge, the Government use license has never been employed as you propose, as a blanket measure to facilitate direct competition with a commercial licensee.
Granting Rights to WHO
In principle, the U.S. Government can license patent rights to the WHO. Even if the doubts regarding WHO’s authority to practice inventions under the Government use license could be overcome, I do not believe that the lack of such a license from the NIH is inhibiting developing countries from addressing their needs. As you stated, many of these countries can issue compulsory licenses, and those that not enacted that authority to date can do so if they choose. The economies of scale you mention could be achieved by cooperation among these countries or direct interaction with WHO. The role of NIH in these sovereign matters is, appropriately, extremely limited.
2001 WARF Stem Cell case.
DHHS used its authority to exercise March-In rights for patents on stem cell lines resulting from publicly funded research and held by the Wisconsin Alumni Foundation (WARF) as leverage to secure an open license on those patents.
- September 5, 2001 press release: National Institutes of Health and WiCell Research Institute, Inc., Stem Cell Research Agreement.
- September 5, 2001. Memorandum of Understanding between WiCell Research Institute, Inc. and Public Health Service U.S. Department of Health and Human Service
2001 Request to HHS to permit the WHO to use inventions funded by the NIH
March 28, 2001 letter from Ralph Nader, James Love and Robert Weissman to Secretary of HHS Tommy Thompson.
We are writing to request that the Department of Health and Human Services (DHHS) enter into an agreement that would enable the World Health Organization, UNICEF and other public health organizations to use US government rights in patents on medicines and other health care inventions.
July 6, 2001 Reply from DHHS Secretary Tommy G. Thompson
I am uncertain how permitting WHO, UNICEF and other international organizations to use “U.S. government rights in patents on medicines and other health care inventions,” as you request in your letter, will advance the agenda of helping developing nations respond to epidemic infectious disease. The massive challenges nations in sub-Saharan Africa and elsewhere face in containing the spread of HIV.AIDS, tuberculosis, and malaria are not created by patent systems or by patents, and solutions do not lie in the area of patent policy.
July 23, 2001 Letter from Ralph Nader to WHO Director General Gro Harlem Brundtland.
US BAYH-DOLE RIGHTS IN PATENTS
For two years, the WHO has hesitated when asked to make an official request to the US government for the right to use US government interests in patents, which is permitted under the US Bayh-Dole Act. WHO officials were reluctant to make this request on the grounds that it would anger big pharma companies. As a consequence, the WHO has no mechanism to obtain inexpensive versions of many drugs that were invented under a government grant, for which the US government could grant licenses for use in poor countries. Also, the WHO has no mechanism to use US government funded research tools. We raised the US Bayh-Dole rights issue as a priority for the new Bush Administration, as did the Trans-Atlantic Consumer Dialogue and many public health groups. On July 6, 2001 US Secretary of Health and Human Services Tommy Thompson wrote to reject our request that the WHO and other UN agencies have access to US rights in government subsidized patents. This rejection was likely due in part to the lack of interest shown by your own staff in acquiring such rights.
2002 Berkeley HeartLab case
On November 11, 2002, Berkeley Heartlab petitioned Spencer Abraham, the Secretary of Energy, “for relief under the Government’s march-in rights or appeal process from an improper licensing decision made because of a conflict of interest.” According to the petition:
BHL requests that the Department of Energy provide it a license to the technology at issue on commercially reasonable terms, whether in the form of an exclusive license, a partially exclusive license, or a nonexclusive license.”
The dispute involved “IB-1730 technology” which “represents a method for determining lipoprotien subsclasses,” that former employees of LBNL obtained a license to commercialize, through a new company, CardioProfile, Inc.
Berkeley Heartlab was later acquired by Celera and is now owned by Quest Diagnostics. There is a glowing LBNL profile of Berkeley Heartlab here. The company has also been involved in legal trouble over marketing practices.
2004 March-in case for the patents on the standalone version or ritonavir sold as Norvir.
In December 2003, Abbott raised the price of its stand alone version of ritonavir, sold under the brand name, Novir, by 400 percent. Essential Inventions shortly thereafter announced it would pursue a march-in case with the NIH.
The 2004 Ritonavir march-in request remains the only march-in case to have the benefit of a public hearing. The patent holder ended up rolling back a 400 percent price hike on Norvir for federal programs. Former Senator Birch Bayh, then working for a law firm that represented Abbott, testified at the hearing, supporting Abbott.
The Essential Inventions petition for the march-in was filed on January 29, 2004. Essential Information proposed that generic drug manufactures provide Abbott with a 5 percent royalty for use of the patents, and also be required to make contributions to a fund to invest in research, thus off-setting any negative impact on R&D from the lower prices for ritonavir. The proposed contributions to the R&D fund were as follows:
- For the US and other countries designated by the World Bank as High Income, $.004 per milligram.
- For countries designed by the World Bank as Low Income, the minimum contribution is zero.
- For countries designed by the World Bank as middle income, the minimum contribution should be $.004, multiplied by the ratio of the country per capita income divided by the average per capita income of the countries designed by the World Bank as high income.
Faced with the march-in request, Abbott offered to rollback the price hike for Norvir for federal programs, then accounting for roughly 70 percent of patients receiving antiretroviral drugs for HIV, and action that clearly influence the NIH.
On July 2, 2004, Elias A. Zerhouni, then Director of the NIH and more recently an employee of Sanofi, rejected the march-in request, suggesting the FTC would be the appropriate body to address the anticompetitive aspects of the Abbott price hike for Norvir, and that more generally:
“the issue of drug pricing has global implications and, thus, is appropriately left for Congress to address legislatively.”
For more background, see:
- Essential Information’s web page on the case.
- 2012. Blog focusing on Birch Bayh’s competing interests and evolving views, August 24, 2012,
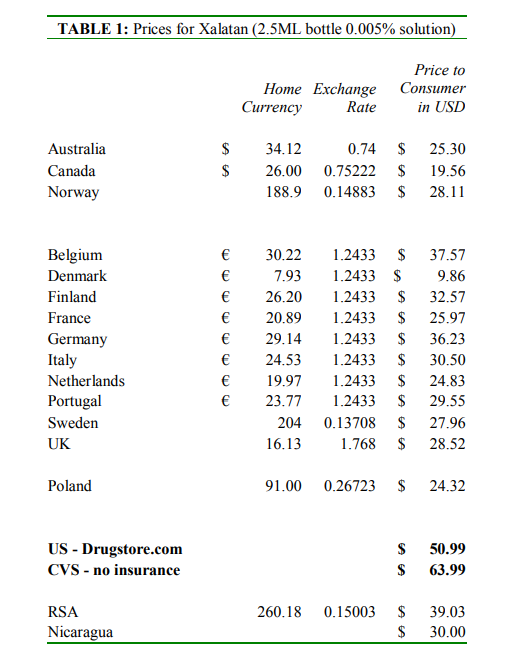
2004, Latanoprost (Xalatan) patents march-in case
File on January 29, 2014, the Essential Inventions petition for march-in rights for the latanoprost patents was overshadowed, at the time, by the ritonavir petition, which was filed on the same day. The latanoprost petition noted that Pfizer was selling latanoprost under the brand name Xalatan in the United States at prices that were two to five times higher than the prices in 13 high income countries. See Table 1 from the Petition.
{kind=link}
Like the ritonavir/Norvir petition, Essential Inventions proposed that generic manufacturers pay the patent holder a royalty, and make a mandatory contribution to an R&D fund. The petition proposed a 5 percent royalty to the patent holder, and a contribution to a fund for neglected R&D equal to $5 per 2.5ML bottle in high income countries, and an amount adjusted for relevative per capita incomes, in middle income countries.
On Sept 17, 2004, Elias Zerhouni, then the Director of the NIH (more recently with Sanofi), rejected the Essential Information march-in petition for the lantanoprost patents.
. . . the record in this instance demonstrates that Pfizer has met the standard for achieving practical application of the applicable patents by its manufacture, practice and operation of latanoprost and the drug’s available and use by the public. . .
Zerhouni rejected the argument that “available to the public on reasonable terms” means “the product should be available at the same price as that charged in other countries.” Also stating “The issue of whether drugs should be sold in the United States for the same price as they are sold in Canada and Europe has Global implications and, thus, is appropriately left for Congress to address legislatively.”
- January 29, 2004 letter to Tommy Thompson, Secretary of HHS, and Petition to use authority under Bayh-Dole Act to promote access to latanoprost, supported by U.S. Public Health Service Research Grant Numbers EY 00333 and EY 00402 from the National Eye Institute, Department of Health and Human Services.
- Sept 17, 2004 decision by Elias Zerhouni rejecting the march-in petition for the lantanoprost patents.
- Essential Information’s web page on the case.
- May 25, 2004 memo by David Halperin. DH.2004NorvirMtg
- May 25, 2004 testimony of Professor Jerome Reichman. Reichman-Norvir-05252004
2006 Reverse genetics patents
The Centers for Disease Control threatened to use March-In rights to issue compulsory licenses on one or more patents on reverse genetics, for use by third parties to manufacture vaccines for avian flu.
2007 OMB request on HIV drugs (royalty free rights)
On January 5, 2007, Essential Inventions requested Robert Portman, Director of the Office of Management and Budget, to take steps to develop and accept alternative competitive sources of supply for federal procurement of two HIV-AIDS medicines: stavudine/d4T and ritonavir. Due to public funding for the development of both drugs, the US government has a royalty free, nonexclusive, worldwide statutory license to the patents for each product. On March 1, 2007, Essential Inventions met with OMB officials, and extended the proposal to include the AIDS drug emtricitabine (Emtriva).
2010 Fabrazyme March-in case
On August 2, 2010, Joseph M. Carik, Anita Hochendoner, and Anita Bova asked the Secretary of DHH to exercise Bayh-Dole march-in rights and grant an open license to use patents related to the manufacture of Fabrazyme (INN: agalsidase beta), an enzyme replacement therapy then sold by Genzyme, a company later acquired by Sanofi. The grounds for the request were that the patent owner and its exclusive licensee have harmed the public health by severely rationing the supply of agalsidase beta, the only approved therapeutic treatment for Fabry disease. The patients were represented by Alan Black. On December 1, 2010, Francis Collins, as Director of the NIH, rejected the march-in petition. However, the NIH continued to monitor the supply shortage and relevant patent litigation in Europe, particularly in Germany, and forced the patent holder, now named the Icahn School of Medicine at Mount Sinai, to end efforts to enforce an injunction against Shire for the manufacturer and sale of Replagal (agalsidase alfa) as a competing treatment in Europe. Shire had previously been barred from selling Replagal in the United States by the Orphan Drug Act exclusive rights obtained for Fabrazyme. Carl Icahn played an important role behind the scenes in this dispute, as a trustee for the medical school which held the patent and as an investor in Genzyme. Icahn used to Fabrazyme shortage to force a sale to Sanofi, and used part of his profits from the transaction as a large gift that lead to the renaming of the school. Several U.S. patients became ill due to the shortage and one died. Today, the U.S. monopoly is intact, while Europe has competition for the treatments. KEI later asked the FTC to investigate the decision by Shire by abandon its application to enter the U.S market, days after Shire resolved a German compulsory license case by obtaining a license from the Carl Icahn medial school, for sales of Replagal in Europe.
- 2010 Fabrazyme March-In Request
- The 2014 FTC complaint regarding collusion between Shire and Sanofi.
2012 patents for ritonavir and other drugs (march-in, royalty free)
2016 UCLA patents on enzalutamide, Astellas brand name Xtandi (march-in, royalty free)
On January 14, 2016, Knowledge Ecology International (KEI) and the Union for Affordable Cancer Treatment (UACT) submitted a request to the National Institutes of Health (NIH) and Department of Defense (DoD) asking that they exercise their authority under the Bayh-Dole Act to authorize the generic production of an expensive prostate cancer drug. See: https://www.keionline.org/22987. KEI and UACT were asking the NIH use either its royalty-free, non-exclusive license or march-in rights.
On April 22, 2016, Biolyse Pharma offered to sell generic versions of enzalutamide to Medicare and other federal programs for $3 per pill, a discount of about 95 percent compared to the Astellas price of Xtandi to Medicare. See: https://www.keionline.org/23069
On June 20, 2016, NIH Director Francis Collins rejected the march-in/royalty free request. See: https://www.keionline.org/23123
On April 29, 2017, KEI and UACT appealed the Collins decision HHS Secretary Price. The appeal was rejected by Francis Collins on June 7, 2017. See: https://www.keionline.org/23322.
More generally see:
2016 Letter from Congress on March-In rights
51 members of Congress have asked the NIH to use March-In rights to rein in high drug prices January 11, 2016.
2016 letter regarding exports to low cost versions of enzalutamide to developing countries.
56 NGOs sent a letter to Sylvia Mary Mathews Burwell, Secretary, Department of Health and Human Services asking the US Government use its royalty free rights in the enzalutamide (generic name for prostate drug Xtandi) patents to enable export of low cost generic versions developing countries, October 17, 2016.
2017 Zinbryta case (march-in, royalty free, termination right)
Request to use Bayh-Dole rights in Zinbryta patents. The drug was later withdrawn from the market over safety issues.
2017 King Directive
- Senate Armed Services Committee directive on use of Bayh-Dole rights for DoD funded drugs, July 17, 2017.
2019 Clare Love, David Reed, march-in and royalty free right petition to U.S. Army concerning enzalutamide.
This is a petition to use march-in or royalty free rights in patents on enzalutamide, based upon the criteria for unreasonable pricing set out in the 2017 directive by the Senate Armed Services Committee Report for the 2018 National Defense Authorization Act.
- February 4, 2019, Clare Love and David Reed petition to the Army to use march-in or royalty free rights in enzalutamide patents.
Additional links
2017
KEI Briefing Note 2017:1. Bayh-Dole Act and difference between March-In Rights and the world wide royalty free rights in patents
Feb. 24, 2017 Compulsory Licensing Workshop – Panel Discussion, Bayh-Dole Act